Principles and context of personalised care
What is personalised care?
Personalised care is one of the five major, practical changes to the NHS that will take place, as set out in the recently published Long Term Plan. Personalised care means people have choice and control over the way their care is planned and delivered. The six components of the universal model for personalised care are shown below. They are based on ‘what matters’ to people and their individual strengths and needs. More information can be found here.
Personalised care is intrinsically linked with primary care and general practice by promoting a holistic approach, considering psychosocial and socio-economic dimensions of health and illness as well as taking a “what matters to me” not a “what is the matter with me” approach that sees an individual as a whole person and not a disease or a collection of conditions.
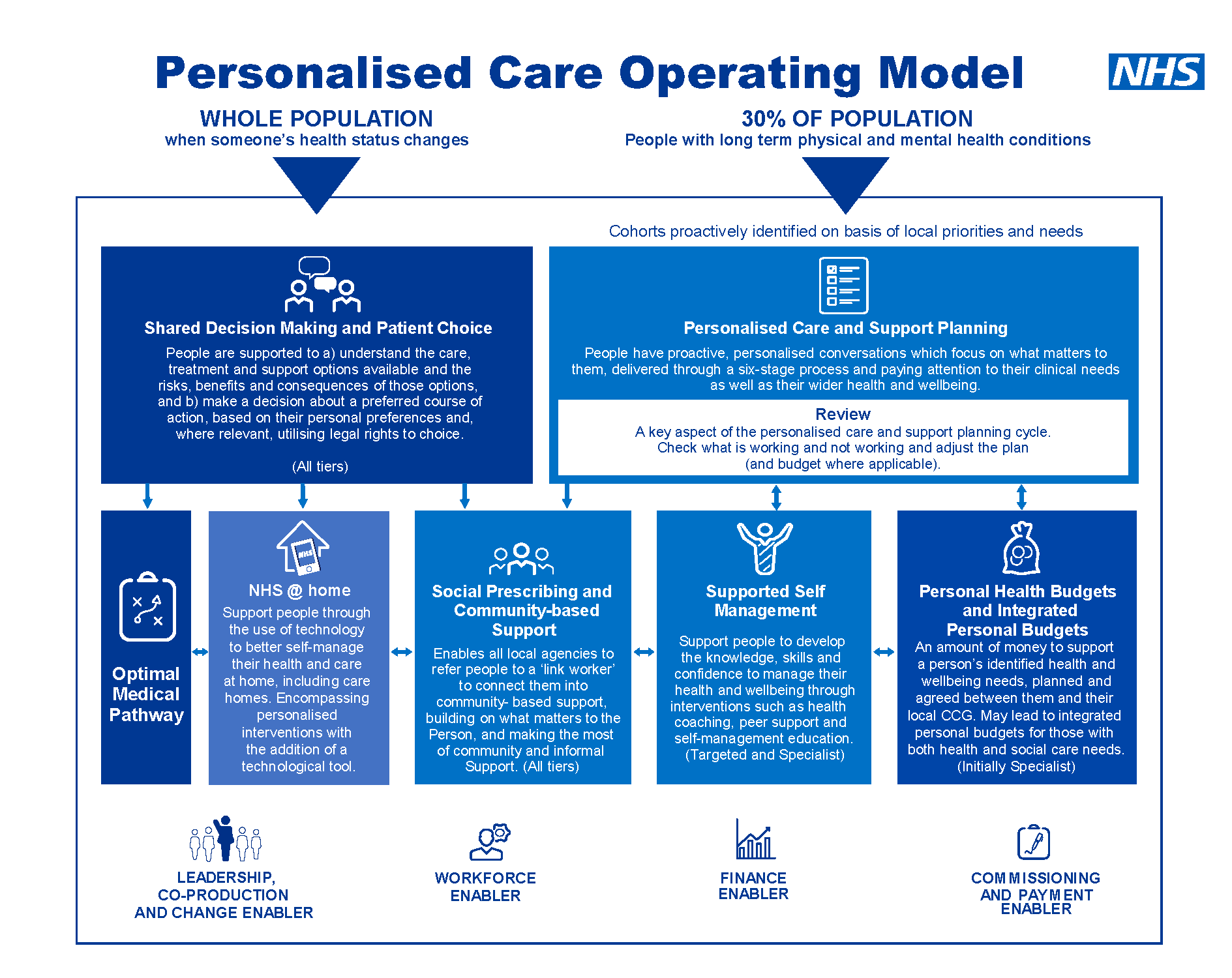
Source: NHS England
Many people working in primary care are familiar with social prescribing, similar approaches have been practised in communities and health care for decades but with patchy provision and a lack of attention by national NHS bodies. Recent years have seen an important shift to embrace, resource and embed social prescribing and personalised care with several key national policies. A list of policies with a summary of key points can be found in Appendix 1. These may be helpful to understand the current policy landscape.
PCNs are seen as anchor institutions with an important role in promoting joined-up care in the community and optimising individual and population health.
The formation of Primary Care Networks is one of the most significant reforms to General Practice in a generation. Their purpose is to:
- Groups local practices together to greater provision of proactive, personalised, coordinated and more integrated health and social care for people close to home
- Improve access to local services for patients with increasingly complex socio-medical problems, GP practices are working together with community, mental health, social care, pharmacy, hospital and voluntary services
- Clinicians describe this as a change from reactively providing appointments to proactively caring for the people and communities they serve.
You can find more information about the Network Contact DES which details core requirements and entitlements of PCNs.
Adapted from Health Creation Alliance
a) Increasing health and social complexity
- People’s health and wellbeing can be affected by a range of social, economic and environmental factors
- People in London are increasingly affected by living with complex long term health conditions, growing unmet health needs and the adverse social determinants of health, the NHS is expanding the Primary Care workforce to help tackle these issues
- Social prescribing, sometimes referred to as community referral, is a way for GPs, nurses and other health care professionals to refer people directly or via a social prescribing link workers (SPLW) to non-clinical services in their local area by focusing on “what matters ” to the patient and taking a holistic approach to health and wellbeing. In particular, it focuses on socioeconomic and psychosocial issues, referred to as the social determinants of health
- The impact will be to reduce the health inequalities people experience and support the clinical workforce experiencing increasing demands.
b) Increasing GP demand
- Increasing GP pressures are widely reported, due to a combination of increasing population size, life expectancy and multi-morbidity, system issues such as increased administrative pressures, and gaps in recruitment and retention placing pressure on the workforce
- Additionally, approximately 20% of GP appointments focus on wider social needs, 4 in 5 GPs report that dealing with non-health issues reduces time to treat patient’s health issues, and two thirds report that dealing with non-health queries increases the stress of their job
- The Inverse Care Law explains that areas with the highest deprivation and patient need are more likely to be under-doctored and resourced, exacerbating unmet need
- Personalised care roles can support the primary care workforce by ensuring that patients get the support they need by the right person, in the right place and at the right time.
c) A responsive personalised care workforce
- In addition to SPLWs, funding for new Personalised Care roles, Health and Wellbeing Coaches (HWBCs) and Care Coordinators (CCs), has been made available to Primary Care Networks through the Additional Roles Reimbursement Scheme (ARRS)
- These roles best work together as part of a “One Team Personalised Care Approach” due to the complementary nature and synergy between their practice; this will be covered in more detail in section 4.11 A One Team Approach for Personalised Care to reduce health inequalities.
Most of the evidence to date has focused on social prescribing, with plans to evaluate the other PC ARRS roles. Evidence demonstrates a range of positive impacts of social prescribing and self-supported management.
| Reduction in | Improvement in |
|
|
Study examples
2017 University of Westminster review
2016 study in Rotherham
2014 study from the University of East London and City and Hackney CCG
|
Links to research and evaluation projects
- The social prescribing academy has an academic collaborative for Social Prescribing evidence, there are reports showing ROI and evaluating SP more generally here.
- A wealth of case studies nationally and in London are available on the Future NHS platform.
- This evaluation about targeting frail patients, shows the ROI of a Care Coordinator or Social prescribing link worker in terms of GP appointment reduction.
- This evaluation about obese or diabetic patients, shows the ROI of Social prescribing link worker in terms of GP appointment reduction.
- Evidence, including research and the social prescribing observatory can be found here.
- HWBC project in SWL
The social prescribing JRSM series has produced the following research outputs:
-
- Reducing chronic stress to promote health in adults: the role of social prescriptions and social movements
- Precision social prescriptions to promote active ageing in older people
- Preparing for COVID-19’s aftermath: simple steps to address social determinants of health
- Digitally enabled social prescriptions: adaptive interventions to promote health in children and young people
- Resetting priorities in precision medicine: the role of social prescribing
- A social prescriptions formulary: bringing social prescribing on par with pharmaceutical prescribing
- Investing resources to address social factors affecting health: the essential role of social prescribing.